
Chapter 14: The Unconscious Patient
Author's Commentary
The content of consciousness is the ability to remember and to utilize and learn new information. The level of consciousness is the degree of alertness or arousal. The reticular activating system is critical for arousal and the cerebral cortex for the content of consciousness. Patients with one functioning hemisphere are completely conscious. Specific deficits of arousal and consciousness can be correlated with lesions of the neuraxis.
Excerpts From Chapter 14
The content of consciousness is the patient’s ability to remember, utilize and learn new information. It is the sum of all mental function. The level of consciousness is the degree of alertness or arousal. In general terms, the reticular activating system is the basis of arousal and the cerebral cortex for the content of consciousness. Full conscious activity requires at least one cerebral cortex and an intact brain stem.
The interplay between the reticular activating system and posterior thalamic and intralaminar nuclei determine the state of arousal. The ascending reticular activity system (RAS), which is important for consciousness, starts in the lateral medulla and receives afferents from all primary senses and the spinothalamic tract. The dorsal pons, periaqueductal gray and intralaminar nuclei of the thalamus are its most important subcortical components. The thalamic intralaminar nuclei have both cholinergic and GABAergic cells that regulate their activity. They project bilaterally to the cortex. Each cortical area is activated by a specific RAS projection. Disruption of the RAS at specific levels causes loss of consciousness or disorders of arousal.
As a general rule, patients with one functioning cerebral hemisphere are completely awake. Therefore, if the cortex is the area suspected of causing lethargy, the problem is usually metabolic, there has been a prior lesion of the other side or there is increased intracranial pressure. Most intracranial problems that alter consciousness do so by pressure on the periaqueductal gray of the midbrain (transtentorial herniation) or by destruction or pressure on the dorsal pons (basilar artery stroke). Thalamic lesions that affect the intralaminar nuclei cause loss of consciousness (acute hemorrhage). Thalamic lesions of the anteroventral (AV) and dorsomedial (DM) nuclei cause waxing and waning of consciousness. Rarely, patients are unconscious from bilateral medullary vascular lesions or trauma. Destructive hemispheric lesions have to be large enough to affect the contralateral hemisphere to cause decreased consciousness. Acute mass lesions cause more disorders of arousal than slowly evolving ones because the brain does not have time to accommodate the new increase of intracranial pressure. Small, strategically placed lesions of the dorsal pons or periaqueductal gray, as well as bilateral brain stem lesions, may cause profound coma.
Examination Technique Demonstration
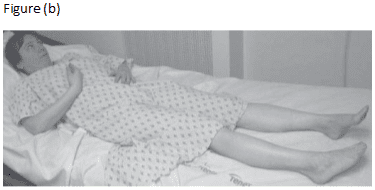
Fig. 14.1 Postures in comatose patients. ….. (b) Decorticate posture. Note the eyes are conjugally deviated to the side of the lesion. The right wrist fingers and arm are flexed and the right foot is slightly dropped and inverted. A left hemispheric lesion.