
Chapter 4: The Motor System
Author's Commentary
The motor system is composed of CNS motor nuclei and their associated modulatory sensory and limbic circuitry.
The major central structures include:
- The primary motor and supplementary motor cortex (M1 and SMA)
- The brainstem reticular formation and pontine nuclei
- Thalamic motor nuclei
- Midbrain
- Spinal step generators
The pyramidal and extrapyramidal systems effect fine movement, maintain tone and posture, and are associated with limbic and motivational circuitry that modifies movement. Sensory feedback is critical at all levels. The cerebellum is essential for coordination, balance, posture, and muscle tone.
The peripheral components of movement are muscles, the neuromuscular junction and joints.
Excerpts From Chapter 4
This is perhaps the most objective component of the neurologic examination. It must be remembered that normal movement depends not only on the reflex arc of the anterior horn cell, the neuromuscular junction, and muscle, but also on intact bones, joints, and soft tissue. This is the foundation upon which supranuclear motor control initiates the “engram," the motor program of movement, its smoothness (cerebellum), its relation to gravity (vestibular system), the control of blood pressure in the upright position (autonomic reflexes) and the desire to move (anterior cingulate gyrus and parietal cortex). Automatic movements for walking (locomotor centers) and for emotion (amygdala, thalamus, and basal ganglia) are clearly important for daily living and have an examination of their own with specific defects that point to specific pathology.
Preliminary General Inspection (Figs 4.1– 4.3)
The aim is to detect specific asymmetries and deformities. This is a combination of genetic defects (dysmorphism) vs acquired lesions. Trophic factors, neuritic outgrowth factors with guidance molecules, and developmental receptors are critical. Congenital abnormalities may lead to overuse syndromes, pressure and destruction of nerve roots as they exit their spinal foramina, as well as stenosis in the cervical and lumbar areas. All the congenital defects can be diagnosed during the neurologic examination.
The patient is evaluated in the supine, sitting, and erect positions. The upper extremities are placed in repose on the lap. A comparison of the size, shape and any adventitial movements is noted.
Examination Technique Demonstration
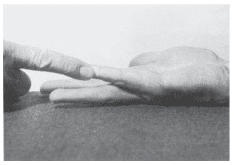
Fig. 4.34
Fig. 4.34 Muscle: abductor digiti minimi. Main segmental supply: T1. Peripheral nerve: ulnar. Test: the back of the hand is placed on the table, and the little finger abducted against resistance (see also Fig. 4.22). Often the only sign of an ulnar lesion.