
Chapter 5: Abnormalities of Posture, Stance, and Spinal Movement
Author's Commentary
Standing and walking are complicated and require sensory input from proprioception, vision, and vestibular nuclei. The circuitry is complex and has cortical, basal ganglia, midbrain, cerebellar and spinal components (step-generators).
Specific gaits are diagnostic of specific disorders from alterations of these circuits. Nuclei important for posture include the vestibular, the medullary and pontine reticular formation, the pedunculopontine nucleus, and the basal ganglia. The medial frontal cortex, supplementary motor area, and paracentral lobule are components of the central control of gait. Peripheral disorders of the spine modulate gait and posture.
Excerpts From Chapter 5
Abnormalities of Posture, Stance and Spinal Movement
Bradykinesia
This physical sign is characteristic of Parkinson's disease and all akinetic rigid syndromes. The movement is slow, its initiation is delayed, and there are no or minimal spontaneous movements. Normal eye blinks are 14 per minute. A bradykinetic patient may blink less than seven times a minute, which frequently simulates a serpentine stare. There is difficulty and decreased turning in bed. Spouses complain that the patient is in the same position in bed in which they went to sleep. Patients have difficulty in changing motor programs. This is often noted when passing through a doorway. The patient freezes and then utilizes small, cautious steps to change direction.
A stooped position (Fig. 5.1)
In diseases of the basal ganglia, the patient has flexed truncal posture, increased flexion of the arms, and a forward flexed head. If the head is extended and the nasolabial folds are deep with flexed arms, the patient has progressive supranuclear palsy. The hands are flexed at the metacarpophalangeal joint in all basal ganglia disease. As Professor Spillane notes*, “Patients that are tall, old, have poor muscular development and overbearing relatives may have stooped posture." The head may fall forward on the chest in severe motor neuron disease, myasthenia gravis, and polymyositis. All elderly patients have a forward flexed neck resulting from cervical spondylosis (“spondylitic neck posture") caused by arthritic degeneration of the uncovertebral joints and desiccation of the cervical disks. If this process is severe, the examiner must be aware that it will be associated with:
- Inability to tandem walk (compression of the laterally placed dorsal and ventral spinocerebellar tracts)
- An inverted radial or supinator reflex at C5–C6
- Hyperactive knee jerks
Examination Technique Demonstration
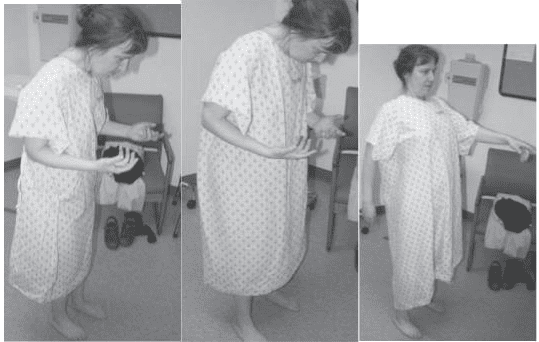
Fig. 5.1 (a), Fig. 5.1 (b), Fig. 5.1 (c)
Fig. 5.1 (a) Normal pressure hydrocephalus (NPH) with forward flexed posture, increased carrying angle of the arms with a normal base. (b) Parkinsonian shuffling, broad-based gait; stance is increased. (c) Martinette gait of alcoholic patient with anterior vermis degeneration. Patients have an extended spine.