Chapter 8: Common Patterns of Abnormal Sensation
Excerpts From Chapter 8
Total Unilateral Loss of All Forms of Sensation
This occurs in the great majority of cases with lesions of the thalamus (ventral posteromedial and posterolateral thalamic nuclei (VPM and VPL)) or as a posterior one-third of the internal capsule lacunar stroke. If this is the case, there is an updraft of the arm with a thalamic hand (adduction and the flexion of the fingers) or a parietal updraft with undulating movement of the fingers (polyminimyoclonus). No extremity moves with normal facility, with absent proprioceptive feedback to the motor cortex. There is a loathness to move with thalamic or parietal lesions, although strength may be intact. In thalamic lesions, motor function may return prior to complete sensory restitution. Rarely, an SI lesion may cause devastating loss of all primary modality sensation on the contralateral side of the body (Fig. 8.1). Another site for this sensory deficit is a partial lesion of the thalamus (VPL and VPM primarily), or a lesion of the upper brain stem that occurs in the dorsal pons, but will be accompanied by cranial nerve deficits and a contralateral hemiparesis. If it occurs with a thalamic lesion, the leg is often affected first and the motor deficit most often clears prior to the sensory deficit. At the red nucleus level of the midbrain, a rubral tremor or postural kinetic tremor will be associated. The spinothalamic-mediated sensations of pain and temperature are dorsal to the red nucleus, while proprioception and lemniscal sensation are lateral. The third nerve nuclear complex is medial to the red nucleus and in the same arterial territory of the thalamic intrapeduncular artery that arises from the tip of the basilar artery and is often involved by a cardiac embolus. Thus, a third nerve lesion associated with spinothalamic sensory loss would suggest a midbrain lesion.
Examination Technique Demonstration
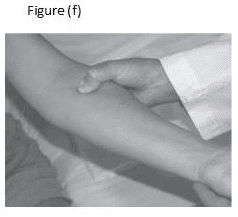
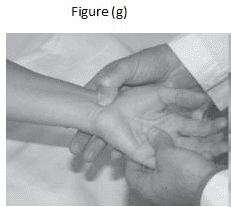
Fig. 8.4 Compression of the upper trunk and entire plexus at the intraclavicular foss and neurovascular bundle. …. (f) The pronator canal. The median nerve enters the forearm between the heads of the muscle and a tight aponeurosis. (g) The carpal tunnel. The median nerve may be sensitized by higher lesions in the brachial plexus. (h) Guyon’s canal. The ulnar nerve lies next to the periform bone at this point.